INTRAARTICULAR SHOULDER PROCEDURES
Indications
Intraarticular shoulder injections are used for diagnostic as well as therapeutic purposes. Corticosteroids and hyaluronic acid are the most commonly injected medications to relieve pain and inflammation or improve lubrication in the joint. Some of the common indications for intraarticular shoulder injections include:
- Arthritis
- Frozen shoulder
- Rotator cuff injuries
- Impingement syndrome
- Tendonitis
- Ligament injuries and Bursitis
Procedure
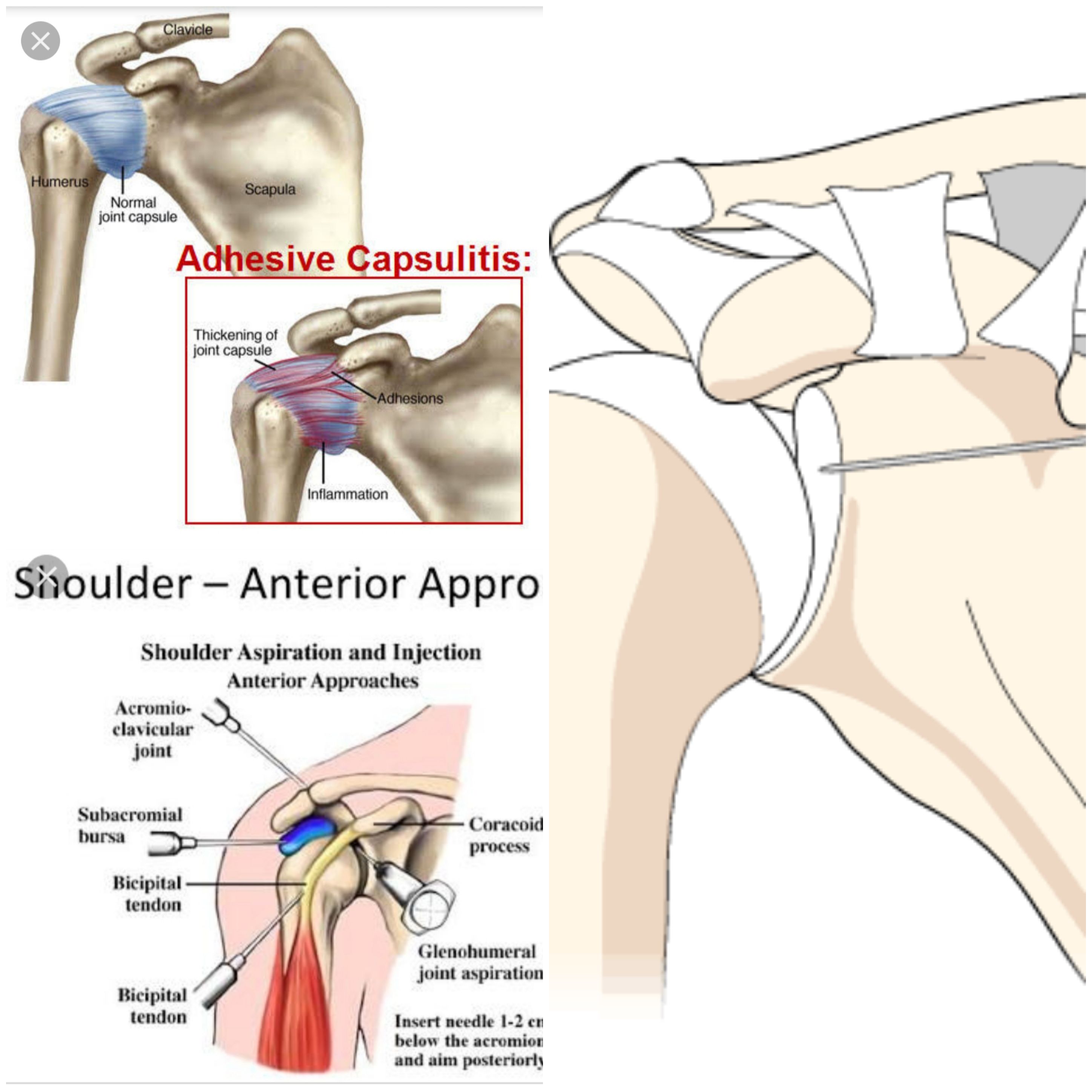
Glenohumeral joint injection
Used for pain relief of shoulder arthritis and frozen shoulder affecting the shoulder. The needle is inserted medial to the head of humerus, lateral to the coracoid process by 1cm and directed posteriorly at a slight superior and lateral angle. Again, an 18 gauge needle should slip into the joint completely and the injection have no resistance.
Subacromial Space injection
Used for pain relief of subacromial impingement / bursitis (subdeltoid bursitis), rotator cuff impingement or tendinosis . The patient sits with their arm resting by their side, as above. The posterior edge of the acromion is recognised, then the needle is inserted inferior to the posterolateral acromion and directed laterally into the subacromial space, aiming for the anterolateral corner of the acromion. A long 18 gauge needle should 2-3cm anterior to the posterolateral corner of the acromion and the syringe plunger should push easily with no resistance during injection. If any resistance is encountered, the needle should be with drawn and readjusted aiming more superiorly under the acromion, as the common error is to inject into the rotator cuff. This should be avoided due to the proteolytic nature of corticosteroids.
Acromioclavicular joint injection
Used for pain relief of osteolysis of the distal clavicle and osteoarthritis of the joint. The patient sits with their arm resting at their side. The distal aspect of the clavicle is palpated to identify the convexity of the AC joint where the clavicle meets the acromion, then the needle is inserted from an anterior and superior angle and directed inferiorly. Over half of the population have an angled AC joint, so a medial direction of the needle will ensure this angle is accounted for. Again, the needle should pass easily into the joint and 2ml injected. The joint will not accommodate more than 2ml.
Long Head of Biceps (LHB) injection
Used for pain relief of biceps tendonitis where the long head of biceps is inflamed This should be preformed under ultrasound guidance, as the biceps tendon is deep under the thick deltoid and impossible to 'feel' with the needle. Injecting the biceps tendon with a proteolytic steroid can also increase the risk of tendon rupture. Therefore, we prefer to use a hyaluronan in young patients. The patient sits with their arm resting by their side. Due to the great variation in humeral version, the tendon position can only be judged by rotating the arm into the best position for injection and letting the patient rest it their. The LHB tendon and groove are identified and marked on the skin with a marker. The point of injection, just lateral to the ultrasound probe is marked. The needle is directed at a 45 degree angle in the long axis of the probe, heading towards the LHB sheath and tendon. The actual tendon is not injected but rather the swollen sheath around the tendon. The injected fluid can be seen to run into the sheath.
Special Instructions
- After receiving the injection, you will remain in the supine or seated position for a few minutes.
- The joint is put through a passive range of motion.
- You will be monitored for about half an hour and may then return home.
- You should avoid strenuous activities involving the injected area for at least 2 days.
- You may experience worsening symptoms initially which can be treated with ice and medications.
- Your doctor will see you in about 3 weeks to check on your progress.
Side Effects And Complications
Intraarticular shoulder injections are a relatively safe procedure. However, it may rarely be associated with certain risks and complications such as:
- Septic arthritis
- Bleeding at the site of insertion
- Injury to adjacent structures
- Pain and swelling
- Infection
- Allergic reaction
Procedures
- EPIDURAL STEROID BLOCK ( TFESI, CAUDAL, INTERLAMINAR )
- CERVICAL EPIDURAL NEUROPLASTY
- INTRAARTICULAR FACET BLOCKS
- MEDIAL BRANCH RFA FOR FACETOGENIC PAIN
- THIRD OCCIPITAL NERVE BLOCKS AND RFA
- C0-C1 and C1-C2 BLOCKS
- OCCIPITAL NERVE BLOCKS AND RFA
- SACROILIAC JOINT BLOCKS and RFA
- GASSERIAN RFA FOR TRIGEMINAL NEURALGIA
- BALLOON COMPRESSION FOR TRIGEMINAL NEURALGIA
- INTRAARTICULAR SHOULDER PROCEDURES
- PROLOTHERAPY
- PRP THERAPY
- GENICULAR NERVE RFA FOR KNEE PAIN
- LUMBAR SYMPATHECTOMY FOR LOWER LIMB ISCHEMIA & CRPS
- T2-T3 GANGLION NEUROLYSIS FOR UPPER LIMB ISCHEMIA AND CRPS
- STELLATE GANGLION BLOCKS AND RFA
- TRIGGER POINT INJECTIONS
- INTRARTICULAR TMJ PROLOTHERAPY
- KNEE JOINT INJECTIONS INCLUDING VISCOSUPPLEMENTATION
- CELIAC PLEXUS BLOCKS AND NEUROLYSIS
- SUPERIOR HYPOGASTRIC PLEXUS BLOCKS AND NEUROLYSIS
- GANGLION IMPAR BLOCK AND RFA