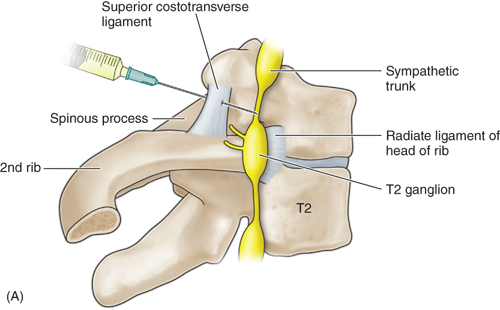
T2-T3 GANGLION NEUROLYSIS FOR UPPER LIMB ISCHEMIA AND CRPS
Indications
- Complex regional pain syndrome 1 and 2
- Herpes zoster (shingles)
- Postherpetic neuralgia (early)
- Postradiation arteritis
- Neuropathic pain associated with CNS pathology
- Phantom limb pain
- Angina pectoris
Procedure
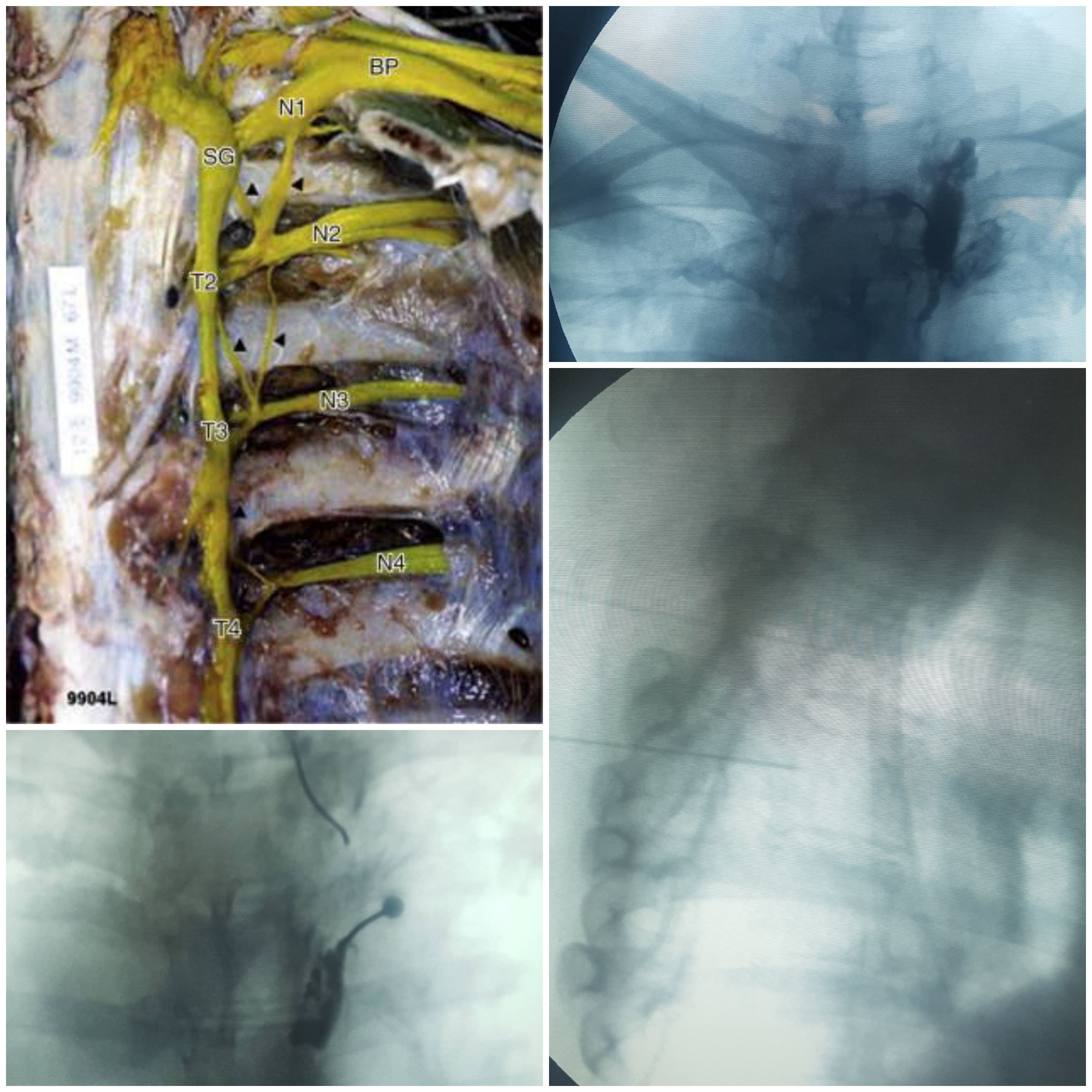
Prophylactic intravenous antibiotics 20 minutes before the procedure are recommended. Place the patient prone on the table. Place a pillow under the chest to fl ex the thoracolumbar spine. The patient head is turned to the side, with the arms resting adjacent to the body. Obtain an intravenous access through a large vein. Before the procedure 500 �1000ml of electrolyte solution should be administered. Administer oxygen by nasal cannula. Monitor the vital signs noninvasively throughout the procedure. Prep and drape the area in a sterile fashion. Sedation may be used to relax the patient; however, the patient should be awake enough to respond to the physician�s questions. The C -arm is placed in the anteroposterior position fi rst to visualize the C7 �T1, T2, T3 vertebral bodies. Rotate the C -arm oblique about 20 � toward the ipsilateral side, then move in a cephalocaudal direction approximately 20� to open the intervertebral space of the T2 vertebral body. The tip of the triangle formed by the T2 vertebral body and the third rib is the target point. Infiltrate the skin with 1% lidocaine at the entry point on the skin at the lateral edge of the T2 vertebral body just cephalad to the third rib. Advance the needle under tunneled vision through the entry point toward the target until it has bony contact with the vertebral body. The needle should always stay in close contact with the lateral edge of the T2 vertebral body. Position the C -arm laterally and advance the needle until the posterior half of the T2 vertebral body. Position the C -arm again to the PA position to confirm that the needle is hugging the T2 vertebral body. After confirming the needle position, inject 2 ml of contrast solution. The contrast solution should not spread into the pleural space and illuminate the dome of the lung. If this happens, remove the needle and redirect. For a diagnostic or prognostic block inject 5 ml of a mixture of 40 mg/ml triamcinolone and 0.5% bupivacaine. In cancer patients, 5 ml of 6% phenol in glycerine for neurolysis can be injected.
Special Instructions
Side Effects And Complications
- Pneumothorax
- Inadvertent puncture of intercostal artery and veins The thoracic sympathetic pain is in close proximity to the intercostal artery and veins. An aspiration test is mandatory before injecting any solution.
- Neuritis of the intercostal nerve
- Other complications
Inadvertent puncture of the thoracic ductus, thyroid gland, trachea, or esophagus are very rare complications that should not occur with the appropriate use of fluoroscopy.
Procedures
- EPIDURAL STEROID BLOCK ( TFESI, CAUDAL, INTERLAMINAR )
- CERVICAL EPIDURAL NEUROPLASTY
- INTRAARTICULAR FACET BLOCKS
- MEDIAL BRANCH RFA FOR FACETOGENIC PAIN
- THIRD OCCIPITAL NERVE BLOCKS AND RFA
- C0-C1 and C1-C2 BLOCKS
- OCCIPITAL NERVE BLOCKS AND RFA
- SACROILIAC JOINT BLOCKS and RFA
- GASSERIAN RFA FOR TRIGEMINAL NEURALGIA
- BALLOON COMPRESSION FOR TRIGEMINAL NEURALGIA
- INTRAARTICULAR SHOULDER PROCEDURES
- PROLOTHERAPY
- PRP THERAPY
- GENICULAR NERVE RFA FOR KNEE PAIN
- LUMBAR SYMPATHECTOMY FOR LOWER LIMB ISCHEMIA & CRPS
- T2-T3 GANGLION NEUROLYSIS FOR UPPER LIMB ISCHEMIA AND CRPS
- STELLATE GANGLION BLOCKS AND RFA
- TRIGGER POINT INJECTIONS
- INTRARTICULAR TMJ PROLOTHERAPY
- KNEE JOINT INJECTIONS INCLUDING VISCOSUPPLEMENTATION
- CELIAC PLEXUS BLOCKS AND NEUROLYSIS
- SUPERIOR HYPOGASTRIC PLEXUS BLOCKS AND NEUROLYSIS
- GANGLION IMPAR BLOCK AND RFA