INTRAARTICULAR FACET BLOCKS
Indications
Facet arthropathy with axial low back pain

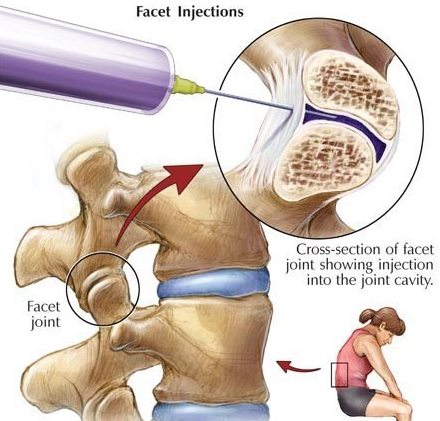
Procedure
Joint between superior articular process of the vertebra below and the inferior articular process of the vertebra above. The facet joints are synovial joints; Articular surfaces are lined by hyaline cartilage and covered by fibrous capsules (1 mm thick).
Volume capacity of these joints: 1.0 to 1.5 ml Lumbar region 0.5 to 1.0 ml Cervical region
NERVE SUPPLY OF FACET JOINT
The sensory innervation of the facet joints comes from medial branch at the same level and one level above
- CERVICAL region: Nerve roots exit the foramen above the vertebral body of same level, thus C4-C5 facet joint receives its innervation from C4 and C5 medial branches
- THORACIC region: Nerve roots runs across the transverse processes one level below i.e, T4 runs across the transverse process of T5, thus T4 T5 facet receives its supply from T3 and T4 medial branches.
- LUMBAR region: Similar to thoracic region.
PAIN DISTRIBUTION OF VARIOUS FACET JOINTS
- Cervical facet pain usually refers to suboccipital, cervical , suprascapular and interscapular regions
- Thoracic facet pain refers to interscapular and surrounding paravertebral region
- Lumbar facet pain to flank, hip, groin, (posterior , lateral & anterior) thigh, lateral calf.
Patient preparation before the procedure
The type of analgesia or sedation needs to be ascertained before performance of the invasive procedure. Place the patient prone on the table. Place a pillow under the abdomen to flatten the lumbar lordosis. An intravenous cannula is inserted for medication injections. Monitoring of vital signs is mandatory. The area for needle entry is prepared in a sterile fashion.
Visualization
Place the C arm in a posteroanterior position first. Identify the midpoint of the intervertebral space at the target level. Adjust the lower endplate of the target vertebral body to be aligned by moving the C arm in cephalocaudal direction. Turn the C arm in the oblique direction approximately 45 degree for L4 and L5 and L5 and S1 levels, and 30 degree for upper levels, until the facet joint comes into view. One should be able to view the Scottie dog in this position. Advance the needle under fluoroscopic guidance in a tunnelled vision fashion toward the inferior aspect of the facet joint to pass the inferior subscapular recess. Another method of gaining intracapsular entry is to redirect the needle slightly medial or lateral to the posterior joint line so that the needle gains access via its medial placement to the insertion of the capsule on the articular process. Inject 0.2 ml of contrast solution to confirm placement . After confirming the correct position of the needle, inject 0.5 ml of depo steroid local anesthetic combination for each facet joint.

Special Instructions
After the procedure is completed, the patient needs to be observed for up to 2 hours. Monitoring of vital signs is mandatory. In addition, the pain relief should be objectively documented. After a satisfactory observation, the patient should be discharged with appropriate and adequate instructions given to their escort. Written instructions are preferable for emergencies and are helpful to the patient and their family.
Side Effects And Complications
- Most problems such as local swelling, pain at the site of the needle insertion and pain in the low back are short- lived and self-limited.
- Inadvertent injection- Dural puncture, Subdural injection, Epidural injection. Foraminal injection, Intravascular injection.
- Trauma to Soft tissue, Medial branch, Nerve root or Spinal cord
- Infection- Soft tissue abscess, Epidural abscess, Facet joint abscess, Meningitis, Encephalitis. The incidence of infection is the same as with the other procedures.
- Bleeding- Soft tissue hematoma, Epidural hematoma, Spinal cord hematoma, Neve root sheath hematoma
- Side effects related to the administration of steroids are generally attributed to the chemistry or to the pharmacology of the steroids. The major theoretical complications of corticosteroid administration include suppression of pituitary-adrenal axis, hypocorticism, Cushing�s syndrome, osteoporosis, avascular necrosis of bone, steroid myopathy, epidural lipomatosis, weight gain, fluid retention, and hyperglycemia.
Procedures
- EPIDURAL STEROID BLOCK ( TFESI, CAUDAL, INTERLAMINAR )
- CERVICAL EPIDURAL NEUROPLASTY
- INTRAARTICULAR FACET BLOCKS
- MEDIAL BRANCH RFA FOR FACETOGENIC PAIN
- THIRD OCCIPITAL NERVE BLOCKS AND RFA
- C0-C1 and C1-C2 BLOCKS
- OCCIPITAL NERVE BLOCKS AND RFA
- SACROILIAC JOINT BLOCKS and RFA
- GASSERIAN RFA FOR TRIGEMINAL NEURALGIA
- BALLOON COMPRESSION FOR TRIGEMINAL NEURALGIA
- INTRAARTICULAR SHOULDER PROCEDURES
- PROLOTHERAPY
- PRP THERAPY
- GENICULAR NERVE RFA FOR KNEE PAIN
- LUMBAR SYMPATHECTOMY FOR LOWER LIMB ISCHEMIA & CRPS
- T2-T3 GANGLION NEUROLYSIS FOR UPPER LIMB ISCHEMIA AND CRPS
- STELLATE GANGLION BLOCKS AND RFA
- TRIGGER POINT INJECTIONS
- INTRARTICULAR TMJ PROLOTHERAPY
- KNEE JOINT INJECTIONS INCLUDING VISCOSUPPLEMENTATION
- CELIAC PLEXUS BLOCKS AND NEUROLYSIS
- SUPERIOR HYPOGASTRIC PLEXUS BLOCKS AND NEUROLYSIS
- GANGLION IMPAR BLOCK AND RFA